Blank Official 122 Utah Form
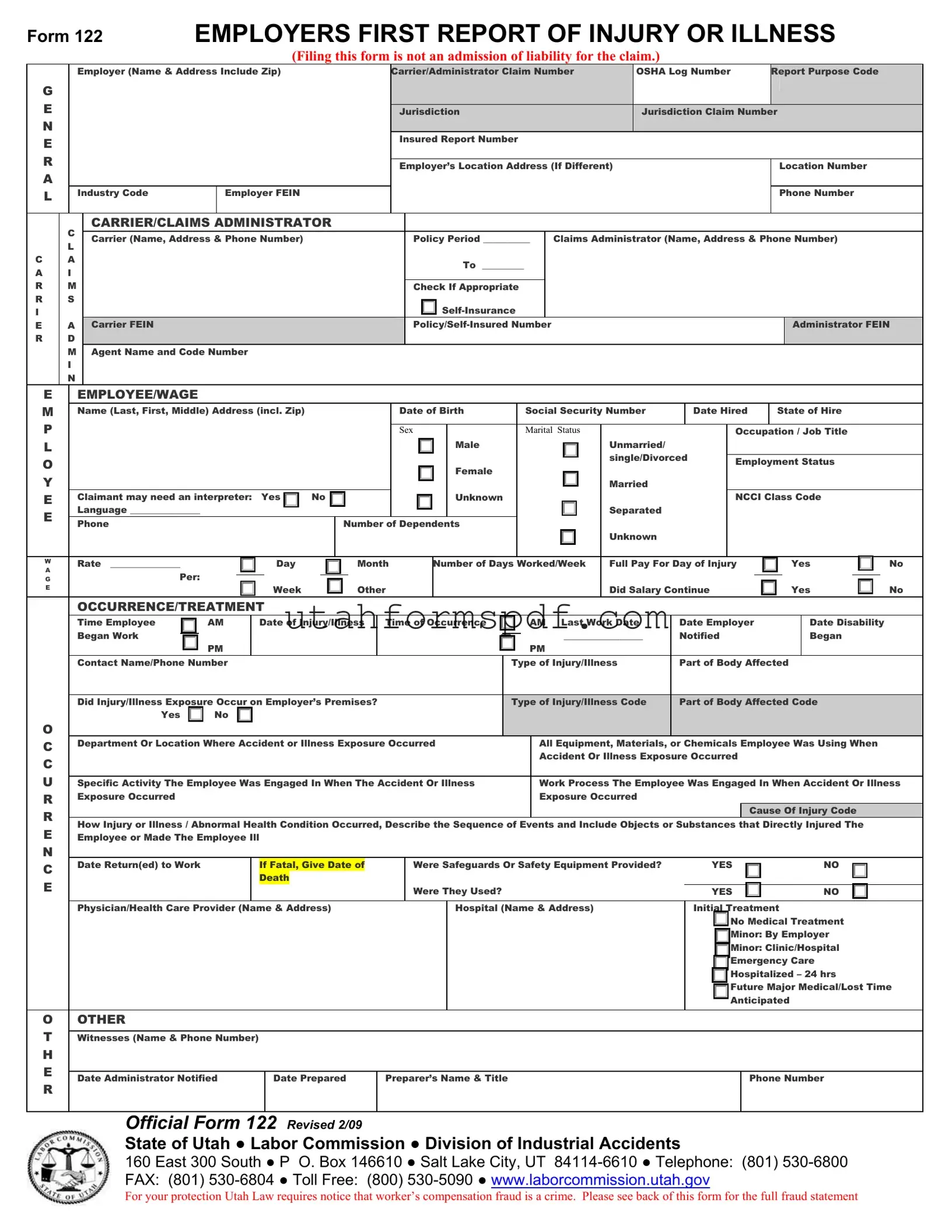
Understanding the intricacies of workplace health and safety is crucial for both employers and employees. In this context, the Official 122 Utah form, also known as the "Employer's First Report of Injury or Illness," serves a pivotal role. This document is designed to streamline the reporting process when an unfortunate incident occurs at the workplace, ensuring that the necessary information is meticulously documented and submitted to the Utah Labor Commission's Division of Industrial Accidents. Essential data captured includes employer and carrier/administrator details, alongside comprehensive information about the employee and the nature of the injury or illness. Prompt filing of this form, within seven days of learning about the incident, aids in expediting the claims process, although it is not considered an admission of liability by the employer. Additionally, the form plays a critical role in worker’s compensation fraud prevention, with stern warnings against presenting false information. It is also a tool for communication, reminding employers to inform injured employees about their rights and possible benefits under Utah’s Workers' Compensation Act. Through carefully outlined instructions, the document ensures that all parties involved are well-informed about their responsibilities, aiming to facilitate a smooth pathway towards recovery and resolution.
Form Preview Example
FORM 122 |
EMPLOYERS FIRST REPORT OF INJURY OR ILLNESS |
|
(Filing this form is not an admission of liability for the claim.) |
G E N E R A L
Employer (Name & Address Include Zip)
Industry Code |
Employer FEIN |
|
|
Carrier/Administrator Claim Number |
OSHA Log Number |
Report Purpose Code |
|
|
|
Jurisdiction |
Jurisdiction Claim Number |
|
|
|
|
Insured Report Number |
|
|
|
|
|
Employer’s Location Address (If Different) |
|
Location Number |
|
|
|
|
|
Phone Number |
|
|
|
C A R R I E R
C
L
A
I
M S
A D M I N
CARRIER/CLAIMS ADMINISTRATOR |
|
|
|
|
Carrier (Name, Address & Phone Number) |
Policy Period __________ |
|
Claims Administrator (Name, Address & Phone Number) |
|
|
To _________ |
|
|
|
|
|
|
|
|
|
Check If Appropriate |
|
|
|
|
|
|
|
|
Carrier FEIN |
|
Administrator FEIN |
||
|
|
|
|
|
Agent Name and Code Number
EEMPLOYEE/WAGE
M |
Name (Last, First, Middle) Address (incl. Zip) |
|
|
|
|
|
|
Date of Birth |
|
|
Social Security Number |
|
|
Date Hired |
State of Hire |
|
||||||||||||||||||||||||||||
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
|
|
|
Marital Status |
|
|
|
|
|
Occupation / Job Title |
|
|||||||||||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
Unmarried/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
single/Divorced |
Employment Status |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Married |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
Claimant may need an interpreter: |
Yes |
No |
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
NCCI Class Code |
|
|||||||||||||||||||||||
E |
Language _______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Separated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Phone |
|
|
|
|
|
|
|
|
Number of Dependents |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
Rate _______________ |
|
|
|
|
|
Day |
|
|
|
Month |
|
Number of Days Worked/Week |
Full Pay For Day of Injury |
|
|
|
Yes |
|
|
|
No |
||||||||||||||||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Per: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
G |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
E |
|
|
|
|
|
|
|
|
|
|
Week |
|
|
|
Other |
|
|
|
|
|
|
|
|
Did Salary Continue |
|
|
|
|
|
|
|
Yes |
No |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
OCCURRENCE/TREATMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Time Employee |
|
|
AM |
|
Date of Injury/Illness |
|
Time of Occurrence |
|
|
|
AM Last Work Date |
|
Date Employer |
|
|
|
Date Disability |
|
|||||||||||||||||||||||||
|
Began Work |
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_________________ |
|
|
Notified |
|
|
|
|
|
|
|
|
Began |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Contact Name/Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
Type of Injury/Illness |
|
Part of Body Affected |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
Did Injury/Illness Exposure Occur on Employer’s Premises? |
|
|
|
|
|
Type of Injury/Illness Code |
|
|
Part of Body Affected Code |
|
|||||||||||||||||||||||||||||||||
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
Department Or Location Where Accident or Illness Exposure Occurred |
|
|
|
All Equipment, Materials, or Chemicals Employee Was Using When |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Or Illness Exposure Occurred |
|
|
|
|
|
|
|
|
|
|||||||||||
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
Specific Activity The Employee Was Engaged In When The Accident Or Illness |
|
|
|
Work Process The Employee Was Engaged In When Accident Or Illness |
||||||||||||||||||||||||||||||||||||||||
R |
Exposure Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Exposure Occurred |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause Of Injury Code |
|
||||||||||
How Injury or Illness / Abnormal Health Condition Occurred, Describe the Sequence of Events and Include Objects or Substances that Directly Injured The |
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||
EEmployee or Made The Employee Ill
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
Date Return(ed) to Work |
|
If Fatal, Give Date of |
|
Were Safeguards Or Safety Equipment Provided? |
YES |
NO |
|||||||||
|
|
Death |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Were They Used? |
YES |
|
|
NO |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician/Health Care Provider (Name & Address) |
|
Hospital (Name & Address) |
Initial Treatment |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
No Medical Treatment |
|||||
|
|
|
|
|
|
|
|
|
|
|
Minor: By Employer |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Minor: Clinic/Hospital |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Emergency Care |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Hospitalized – 24 hrs |
|||||
|
|
|
|
|
|
|
|
|
|
|
Future Major Medical/Lost Time |
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Anticipated |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OOTHER
TWitnesses (Name & Phone Number)
H |
|
|
|
|
|
E |
|
|
|
|
|
Date Administrator Notified |
Date Prepared |
Preparer’s Name & Title |
Phone Number |
||
|
|||||
R |
|
|
|
|
|
|
|
|
|
|
OFFICIAL FORM 122 REVISED 2/09
STATE OF UTAH ● LABOR COMMISSION ● DIVISION OF INDUSTRIAL ACCIDENTS
160 East 300 South ● P O. Box 146610 ● Salt Lake City, UT
FAX: (801)
For your protection Utah Law requires notice that worker’s compensation fraud is a crime. Please see back of this form for the full fraud statement
FRAUD – “Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.”
INSTRUCTIONS TO EMPLOYER
The Employer’s First Report of Injury or Illness must be submitted to the Labor Commission, Division of Industrial Accidents, per Sections
*All information requested on this form is of vital importance. Please answer all items in detail in order to avoid additional correspondence or the return of this report for completion. Do not enter data in the shaded areas.
*The box titled “OSHA Log Number” must be filled in with the employer assigned Case Number from OSHA’s new 300 Injury Log. The Case Number needs to reflect the year of the injury – for example, your first injury in 2002 should reflect the first injury and the year 00/02 with the next injury being 00202, etc.
*Please provide WAGE information. This information is needed by the insurance company for paying the correct amount on a claim.
*The injury report on file with the Labor Commission, Division of Industrial Accidents, is private information and is only released to parties to the claim.
*Please make sure the EMPLOYER NAME is correct, as well as your FEIN # (Federal Tax ID Number). The employer’s name should be the same as reported to The Department of Workforce Services and as it appears on your WORKERS’ COMPENSATION insurance policy.
*The Labor Commission is to receive an original of this report, Worker’s Compensation Insurance Carrier gets a second copy, the employee gets a third copy, and the employer gets a fourth copy and should maintain a copy of this report.
*Failure to file this report with the Labor Commission or failure to provide the employee with a copy of the report, is a Class C misdemeanor and can also result in a citation and a civil penalty for each violation as per
*If you dispute the validity of this claim you need to contact your insurance carrier, but you must still file the “Employer’s First Report of Injury or Illness” form with the Labor Commission.
*Reminder: Inform your injured employee of his/her rights and obligations (as outlined on the back of the employee’s copy) of Utah’s Workers’ Compensation Act.
For Additional Information please contact:
State of Utah – Labor Commission Division of Industrial Accidents 160 East 300 South, 3rd Floor
P O Box 146610
Salt Lake City, Utah
FRAUD – “Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.”
EMPLOYEE INFORMATION
•INJURY/ILLNESS REPORT: A report of your injury/occupational illness must be made with your employer. If a report of injury is not filed with your employer or the Labor Commission, Division of Industrial Accidents, within 180 days of the date of your injury/illness, you may lose the right to ever file a claim for workers’ compensation benefits for that injury or illness.
•EMPLOYER’S PHYSICIAN: If your employer has a company physician or designated clinic for industrial accidents, you MUST see the company physician first, or you may not be eligible for workers’ compensation benefits. After you have been seen by your employer’s physician, you have the right to choose one treating physician.
•MEDICAL COOPERATION: You must cooperate with your employer or the insurance carrier in following prescribed medical treatment in order to return to work as quickly as possible.
•TRAVEL REIMBURSEMENT: You may be eligible for travel reimbursement to and from approved medical care. You will need to keep records. Contact your insurance carrier regarding travel expenses.
•REEMPLOYMENT ASSISTANCE: You may be eligible for reemployment assistance if you are unable to return to work due to an industrial injury. Contact your insurance carrier or the Labor Commission, Division of Industrial Accidents, for further information.
•MEDICAL EXPENSES: You are entitled to have all reasonable medical expenses paid that are a result of the injury or illness.
•COMPENSATION BENEFITS: You are entitled to
□If you have sustained a permanent impairment due to the industrial injury or disease, you are entitled to compensation based on the impairment rating as determined by a physician.
□If you are permanently totally disabled from working due to the industrial injury, you may need to apply at the Labor Commission, Division of Industrial Accidents, for a hearing to determine if benefits are due.
•ADDITIONAL ASSISTANCE: If you are unable to work due to an industrial injury and meet the program’s requirements, you may be eligible for other assistance. Agencies you may wish to contact:
□Department of Workforce Services for food stamps, cash assistance, medical assistance, or employment assistance.
□Social Security for total disability benefits.
•UNEMPLOYMENT BENEFITS: If you are able to work, but have been terminated from your job, you need to apply at the nearest Department of Workforce Services employment office within 90 calendar days after you are released from
Contact your insurance carrier if problems occur during your injury regarding payment of medical bills or compensation benefits. If you need to know who your employer’s insurance carrier is, you may ask your employer or contact the Labor Commission, Division of Industrial Accidents.
THIS IS AN IMPORTANT DOCUMENT TO MAINTAIN FOR YOUR RECORDS
Form Breakdown
| Fact | Description |
|---|---|
| Form Purpose | The form is used for employers to report first instances of injury or illness in the workplace. |
| Admission of Liability | Filing the form does not indicate an admission of liability for the claim. |
| Governing Laws | Sections §34A-2-407 and §34A-3-10B, Utah Code Annotated (U.C.A.) 1997. |
| Filing Deadline | Employers must file within seven days after the occurrence or the employee’s notification of the incident. |
| OSHA Log Number Requirement | Employers must fill in the OSHA Log Number with the employer-assigned Case Number from OSHA’s new 300 Injury Log. |
| Confidentiality | The injury report is considered private information, released only to parties to the claim. |
| Copy Distribution | Copies of the report must be distributed to the Labor Commission, the insurance carrier, the employee, and the employer. |
| Penalties for Non-Compliance | Failure to file or provide the employee with a copy can result in a Class C misdemeanor and other penalties. |
| Workers’ Compensation Fraud Warning | The form includes a fraud warning, indicating that worker’s compensation fraud is a punishable crime. |
Detailed Steps for Writing Official 122 Utah
Once an incident occurs that necessitates filing the Official 122 Utah Form, commonly known as the Employer’s First Report of Injury or Illness, it’s crucial to approach the task with attention to detail and a sense of urgency. This form is a vital component in the workers’ compensation process, serving to document the initial details of an employee’s workplace injury or illness. It's not merely a formality but a critical step that ensures the accurate processing and evaluation of the injury or illness report within the stipulated legal framework. Given its importance, it’s imperative that employers fill out this form meticulously and submit it within the required timeframe to avoid any penalties or delays in the employee's compensation claim.
To successfully complete the Official 122 Utah Form, follow these detailed steps:
- Start by accurately filling in the General section. Include the employer's name and address, industry code, Employer FEIN, and if applicable, the carrier/administrator claim number, OSHA log number, report purpose code, jurisdiction, jurisdiction claim number, insured report number, employer’s location address if different, location number, and phone number.
- Proceed to the Carrier Claims Admin section, where you should list the carrier or claims administrator's name, address, and phone number. If relevant, indicate the policy period, check if it's self-insurance, and provide the carrier FEIN, policy/self-insured number, administrator FEIN, and the agent name and code number.
- In the Employee/Wage Information area, detail the employee’s name, address, date of birth, social security number, date hired, state of hire, sex, marital status, occupation/job title, employment status, if an interpreter is needed and the language, NCCI class code, rate of pay, pay frequency, if full pay for the day of injury was provided, and if salary continued post-injury.
- Address the Occurrence/Treatment section by including the time and date of the injury or illness, time of occurrence, the last work date before the incident, the date employer was notified, the date disability began, contact name and phone number, type of injury or illness, part of the body affected, if the incident occurred on the employer's premises, department or location where the incident occurred, all equipment, materials, or chemicals involved, the specific activity and work process the employee was engaged in, cause of injury code, and how the injury or health condition occurred, with a description of the sequence of events.
- Fill in the Recovery/Return to Work section with information about the date the employee returned to work or is expected to, if applicable, the date of death, if safeguards or safety equipment were provided, and if they were used.
- In the Physician/Health Care Provider part, write the name and address of the attending health care provider and the hospital, if applicable, and the initial treatment rendered.
- List any witnesses to the incident, their names and phone numbers, in the Others section.
- Conclude by entering the date the administrator was notified, the date the form was prepared, preparer’s name and title, and phone number.
Once completed, the form must be distributed accordingly: the original goes to the Labor Commission, Division of Industrial Accidents, one copy to the Worker’s Compensation Insurance Carrier, one to the injured employee, and one for the employer’s records. Timely and accurate submission not only complies with Utah law but also supports the well-being of the employee by ensuring a smooth claim process.
Common Questions
-
What is the Official 122 Utah Form?
The Official 122 Utah Form, also known as the Employer's First Report of Injury or Illness, is a document employers in Utah must submit to the Labor Commission, Division of Industrial Accidents following an incident that results in an injury or illness to an employee. This filing is required when the incident involves medical treatment by a physician, loss of consciousness, work restriction, transfer to another job, or loss of work.
-
When must an employer file the Official 122 Utah Form?
An employer is mandated to file the form within seven days following the occurrence of an injury or illness, or after being notified by the employee of such an incident. This timeframe ensures timely processing and support for the affected employee.
-
Is filing the Official 122 Utah Form an admission of liability?
No, filing this form is not an admission of liability for the claim. It is a procedural step required by Utah law to formally report the occurrence of a workplace injury or illness.
-
What information is required on the Official 122 Utah Form?
- Employer and Carrier/Administrator details
- Employee and Wage information
- Details about the occurrence/treatment
- Information about any witnesses
- Physician/Health Care Provider and initial treatment details
All sections must be completed in detail to avoid further correspondence or the return of the report for completion.
-
What are the consequences of not filing the form?
Failure to submit this form to the Labor Commission or to provide the employee with a copy can result in a Class C misdemeanor. Additionally, the employer may face citations and civil penalties for each violation.
-
What should an employer do if they dispute the claim?
If an employer disputes the validity of an injury or illness claim, they must still file the Official 122 Utah Form with the Labor Commission. They should also contact their insurance carrier to address the dispute directly.
-
How can an employee's rights be affected if they do not file a report of injury?
If an injury or illness report is not filed with the employer or the Labor Commission within 180 days of the occurrence, the employee may lose the right to file a claim for workers' compensation benefits for that injury or illness.
-
Where can one find additional information or assistance?
For more information or assistance with the Official 122 Utah Form, contact the State of Utah Labor Commission Division of Industrial Accidents at (801) 530-6800 or (800) 530-5090, or visit their website.
Common mistakes
Filing the Official 122 Utah form, titled "Employers First Report of Injury or Illness," is a crucial step in the workers' compensation claim process. However, inaccuracies or omissions can significantly delay benefits. Here are nine common mistakes to avoid:
- Not Reporting on Time: One of the most common errors is not submitting the form within the seven days after the occurrence or knowledge of the injury or illness that necessitates medical treatment, causes loss of consciousness, results in missed work, or requires a job change.
- Incomplete Employer Information: Failing to provide complete and accurate employer details, including the correct business name, address, and Federal Employer Identification Number (FEIN), can lead to processing delays. Remember, the employer's name should match the one registered with the Department of Workforce Services and on the worker’s compensation insurance policy.
- Omitting the OSHA Log Number: Failure to include the employer-assigned OSHA case number from the new 300 Injury Log can result in the form being returned for completion.
- Inadequate Description of Incident: Not providing a detailed account of the injury or illness, including how it occurred, the specific activities the employee was engaged in, and the materials or substances involved, can cause significant delays in claim processing.
- Vague Injury/Illness Information: Merely stating the type and location of the injury or illness without sufficient detail, or using overly broad terms, can lead to misunderstandings and delays.
- Incorrect or Missing Wage Data: For claims processing, accurate wage information is essential. This includes the rate of pay, the regularity (day, week, month), and whether full pay was provided on the day of the injury.
- Not Providing Safety Equipment Details: Overlooking details about the provision and use of safety equipment can negatively impact the investigation and adjudication of the claim.
- Overlooking Witness Information: Witnesses can provide crucial details about the incident. Not listing their names and contact information can hinder the claim's validation process.
- Failing to Notify about Fatalities or Serious Injuries: Employers must notify the Division of Occupational Safety and Health within 8 hours of a work-related fatality or serious injury, in addition to filing this form. Neglecting this step could result in legal repercussions.
To ensure a smooth and efficient claim process, it’s imperative to pay close attention to detail and complete all sections of the Official 122 Utah form accurately. Furthermore, understanding that this document serves not only as a critical component in the workers’ compensation process but also fulfills reporting obligations under Utah law can underscore the importance of its accurate and timely submission. Employers are encouraged to review the instructions provided with the form carefully and consult with their workers' compensation insurance carrier or a legal professional if they have any questions or concerns about the reporting process. Avoiding these common mistakes can significantly expedite claim resolution and ensure that employees receive the benefits and care they are entitled to without unnecessary delay.
Documents used along the form
When managing a workplace injury or illness in Utah, the Official 122 Form serves as a crucial document for starting the claims process. However, several other forms and documents often accompany this form, each serving a unique purpose in ensuring comprehensive reportage and compliance with Utah's Workers' Compensation Law. Understanding these documents can assist employers, employees, and insurance carriers in navigating the complexities of workers' compensation claims efficiently and effectively.
- Wage Verification Form: This document is used to verify the injured employee's earnings. It provides detailed information about the employee's salary, including hours worked and rate of pay, prior to the injury or illness. This information is vital for accurately calculating workers' compensation benefits.
- Medical Release Form: A signed medical release allows the employer or the insurance carrier to obtain the employee's medical records related to the injury or illness. This ensures that the treatment received is appropriate for the injury claimed and helps in the evaluation of the workers' compensation claim.
- Accident Investigation Report: Often completed by the employer or a designated safety officer, this report details the circumstances surrounding the accident or illness. It includes witness statements, conditions of the work environment at the time of the incident, and any measures taken to prevent future occurrences.
- Choice of Physician Form: In Utah, injured workers have the right to choose their treating physician after initially being seen by the employer’s designated medical provider. This form documents the employee's choice of physician for treating the injury or illness related to their workers' compensation claim.
- Return to Work Form: As the injured employee recovers, a return to work form completed by the treating physician specifies the employee's work restrictions and abilities. This form is critical for employers to safely accommodate the employee’s return to work, potentially in a light-duty capacity until fully recovered.
Together, these forms complement the Official 122 Utah form, creating a thorough and precise record that benefits all parties involved. Employers are encouraged to maintain these documents meticulously, ensuring that both the employee's needs and regulatory requirements are met throughout the recovery and claim process. In managing these documents, respect for the employee's privacy and adherence to legal guidelines should govern all actions.
Similar forms
The Official 122 Utah form, which serves as an employer's first report of injury or illness, shares similarities with the OSHA Form 300, "Log of Work-Related Injuries and Illnesses." Both documents are integral in reporting workplace injuries or illnesses, ensuring that incidents are officially recorded for regulatory compliance and safety analysis. The OSHA Form 300, however, focuses more broadly on logging work-related injuries and illnesses for occupational safety and health monitoring, making it a critical tool for identifying patterns and implementing preventive measures.
Another document akin to the Official 122 Utah form is the DWC Form-001, "Employer's First Report of Injury or Illness," used in Texas. Like the Utah form, it is designed for employers to report instances of workplace injuries or illnesses to the respective state's workers' compensation board. Both forms collect detailed information about the incident, the employee involved, and the employer, but they cater to the specific reporting requirements and regulations of their respective states, highlighting the local nuances in workers' compensation processes.
The CA-1, "Federal Employee's Notice of Traumatic Injury and Claim for Continuation of Pay/Compensation," is a federal form used in similar circumstances as the Official 122 Utah form but specifically for federal employees. It serves a dual purpose: to notify about a traumatic injury and to initiate a claim for benefits. Both documents are critical in the early stages of a workplace injury or illness case, facilitating timely documentation and processing of claims. However, the CA-1 is tailored to the federal workers' compensation system, managed by the Office of Workers' Compensation Programs (OWCP).
Similarly, the "First Report of Injury or Illness" form, which states like Florida use, shares the fundamental purpose of capturing details about workplace incidents that result in injury or illness. This document also helps in navigating the workers' compensation claims process, providing a formal record of the incident. Like the Official 122 Utah form, it's the starting point for any workers' compensation claim and plays a vital role in ensuring the injured or ill worker receives appropriate care and compensation.
Lastly, the "Employer’s Report of Industrial Injury" form used in Arizona parallels the Official 122 Utah form in function and intent. It is required when an employee suffers a workplace injury or illness, marking the beginning of the claims process for workers' compensation benefits. Both documents are essential for legal compliance, serving as an official notification to the state's industrial commission. They ensure that both the incident and the affected employee's details are thoroughly documented, setting the groundwork for any subsequent investigation or compensation claim.
Dos and Don'ts
When filling out the Official 122 Utah Form, it's crucial to follow certain dos and don'ts to ensure proper submission and to avoid common mistakes that could lead to issues with your report filing. Here are seven things you should and shouldn't do:
- Do ensure all the information provided on the form is complete and accurate. Incomplete forms or inaccuracies can often lead to unnecessary delays.
- Do verify the Employer FEIN (Federal Employer Identification Number) and the Employer's Name are correctly entered and match those on record with the Department of Workforce Services and your workers' compensation insurance policy.
- Do include the correct OSHA Log Number, as this helps in identifying the case properly and aligning it with federal and state reporting requirements.
- Do provide detailed wage information as requested on the form. This detail is essential for the insurance company to process claims accurately and timely.
- Do submit the form within seven days after the employee notifies the employer of the injury or illness, as stipulated by Utah law, to avoid penalties.
- Don't leave shaded areas or any sections meant for administrative use blank if applicable to your report.
- Don't forget to distribute copies of the completed form correctly: one to the Labor Commission, one to the Worker’s Compensation Insurance Carrier, one to the injured employee, and one for the employer's records.
Adhering to these guidelines will help streamline the reporting process, ensure compliance with Utah's Labor Commission requirements, and support timely and accurate benefits processing for injured employees.
Misconceptions
The Official 122 Utah form, known as the Employer’s First Report of Injury or Illness, is often misunderstood. Addressing these misconceptions can clarify its purpose and requirements, ensuring better compliance and understanding. Here are eight common misconceptions:
- Filing the form admits liability: Filing Form 122 does not constitute an admission of liability for the claim. Its primary purpose is to report the occurrence of an injury or illness related to the workplace.
- It's optional to file the form: Employers are mandated to submit the form to the Labor Commission, Division of Industrial Accidents, within seven days after the occurrence or notification of an injury or illness that requires medical treatment beyond first aid or leads to lost time from work.
- Only major injuries or illnesses need to be reported: Any injury or illness that results in medical treatment, loss of consciousness, restriction of work, or transfer to a different job must be reported, not just those that are considered major or severe.
- The employer’s insurance information is not necessary: Complete insurance or carrier/administrator information is critical for processing the claim and ensuring that the appropriate parties are notified and engaged in the process.
- The report serves as the sole notification for all workplace injuries or illnesses: In addition to filing Form 122, employers must also notify the Division of Occupational Safety and Health within eight hours of a work-related fatality or significant injury, as defined by the state.
- Employee consent is required to file the report: Employers are required to file this report based on occupational incidents and do not need consent from the employee to do so. However, it is good practice to inform the employee that a report will be filed.
- The form is public information: The injury report filed with the Labor Commission is private information and is only released to parties involved in the claim, ensuring confidentiality and privacy of the affected employee.
- Failing to file the form has no real consequences: Failure to properly file the form not only is considered a Class C misdemeanor but can also result in a civil penalty for each violation, emphasizing the importance of compliance.
Understanding these points about the Official 122 Utah form can help employers navigate the process of reporting workplace injuries or illnesses efficiently and in compliance with state requirements, ensuring both the well-being of employees and the integrity of workplace safety protocols.
Key takeaways
Filling out and using the Official 122 Utah form, known as the Employer's First Report of Injury or Illness, is an essential step in complying with state regulations when an employee gets injured or falls ill due to work. Understanding the correct way to complete and utilize this form not only helps in avoiding potential legal issues but also ensures that the injured employee receives the necessary benefits. Here are four key takeaways:
Timeliness is crucial: The form must be submitted to the Utah Labor Commission, Division of Industrial Accidents, within seven days of the employer being notified of the injury or illness. This prompt action is necessary to comply with Utah Code Annotated (U.C.A.) §§ 34A-2-407 and 34A-3-10B. Delaying this process can lead to penalties and hinder the employee's access to benefits.
Accuracy and Completeness: Every field on the form requires accurate and detailed information to avoid the need for further correspondence or the return of the report for completion. Information such as the OSHA Log Number, accurate wage details, and a thorough description of the injury or illness and how it occurred are essential for processing the claim efficiently.
Privacy Protection: The information provided on the injury report is considered private and is only released to parties directly involved in the claim. It's crucial to ensure all personal and sensitive data is carefully handled and accurately reported to protect all parties' privacy and rights.
Report Distribution: After completing the report, distributions need to be made adhering to specific requirements: the original form should be sent to the Labor Commission, a second copy is for the Worker’s Compensation Insurance Carrier, the third copy is provided to the injured employee, and the employer retains the fourth copy for their records. Maintaining this distribution ensures compliance and assists in the smooth processing of the worker's compensation claim.
It's also important to note that failure to file this report or failing to inform the employee can result in significant consequences, including Class C misdemeanor charges and potential civil penalties. Moreover, if an employer questions the validity of a claim, they must still file the report with the Labor Commission while addressing their concerns with their insurance carrier. Understanding these aspects is fundamental to navigating the process of managing workplace injuries and illnesses within Utah's regulatory framework efficiently and compassionately.
Common PDF Templates
Medical Power of Attorney Utah - Outline specific medical treatments you consent to or refuse, including life-sustaining measures, in your Utah Advance Health Care Directive to ensure your medical values are honored.
Dws-esd 631 - Facilitates the detailed reporting of employee wages to the Utah Department of Workforce Services for unemployment benefit administration.
Utah Tax Forms - Insurance for the special plates must be issued in the name of the licensed business applying for the plates.